Accessibility Options
Go to the PDF of the final report
Text Slides
[googleapps domain=”docs” dir=”presentation/d/e/2PACX-1vS-E5FUAEwxL38wf296e0konEtRPBy3Wl5Xua8yGmyc2HKUWikrkp_kxEpUjSmgu9aOc–oAnpoqtZy/embed” query=”start=false&loop=false&delayms=3000″ width=”800″ height=”498.3″/]Click on the 3 dots below the slides to select the full screen view.
Video
Go to Youtube if you want to select which chapter to watch from the playlist.
A | B | C | D | E | F | G | H | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z
A
Accessible: When people with disabilities can easily use something. A setting or communication must work as well for people with disabilities as it does for everyone else.
Accessibility: What makes it easy for people with disabilities to obtain, understand or use.
Adolescence: Is from 10 to 19 years old. It is the time when a person is growing to become an adult.
Adolescent: A person who is 10 to 19 years old.
Adult Independence: An adult with disabilities is free to make their own day-to-day choices. For example: how to live, work, and take part in their communities.
Adult resources: Information and supports for adults.
Advocate (to): To speak up and make a case for what you need.
Affirmative Resources: Supports that are respectful and welcome a person the way they are.
Aggressive Behaviors: Words or actions that may hurt someone
Anxiety: Intense feelings of worry and fear.
ASAN: The Autistic Self-Advocacy Network is an organization run for and by autistic people.
Attention Deficit Hyperactivity Disorder (ADHD): A condition where someone:
-
finds it hard to pay attention
-
may act without thinking
-
and needs to move a lot
Augmentative Alternative Communication (AAC): Ways, besides talking, that people show others what they want and need. This includes writing, pointing at pictures, typing, using signs, etc.
B
Behavioral Therapy: Therapy to change unhealthy or harmful ways people act.
Behavior Treatments: (See Behavior Therapy)
Bi-Polar Disorder: A disorder where someone’s mood changes between highs and lows.
Blood Draws: Inserting a needle into a vein to collect a blood sample for testing.
C
Capitated: Paying an amount of money based on how many patients are seen at a doctor’s office.
Caregiver: Someone who helps a person with everyday activities.
Case Management: Someone who helps make sure your services and supports work for you.
Community Programs: Activities or supports provided in your town in the same places as people without disabilities.
Community Resource Guide: A list of support services and resources in a local area.
D
Depression: Feelings of sadness or lack of interest in activities you once found enjoyable. It can change how much you sleep or eat.
Developmental disability services: Supports and programs for persons who are disabled before the age of 18.
Dietician: A healthcare professional who helps people eat healthy.
Dual Disability: Having more than one disability.
E
Executive functioning: How your brain works to focus, make a plan, remember and do more than one thing at the same time.
F
Funding: Money from an organization or government.
G
Gastro-intestinal: The many different parts of your body that food and liquid go through. For example: your mouth, stomach, or anus.
Government Policy-Makers: People in government who make rules and laws.
Guardianship: Guardianship is a legal word. Guardianship is when a court decides that a person cannot make their own decisions. The court then appoints someone else to make decisions for the person.
H
Healthcare professionals: People trained to provide healthcare. This includes doctors, nurses, therapists, etc.
Healthcare providers: People or places that provide healthcare. This includes doctors, nurses or hospitals.
Healthcare transition: When teenagers start making their own healthcare decisions as they become adults. They may change to a new doctor for adults.
Healthcare transition supports: Ways to make healthcare transition easier for teenagers and their parents.
Health Maintenance Organization (HMO). A group of doctors and hospitals who accept a set amount of money for services they provide.
Housing: A place where people live.
I
Insurance: A person pays a set amount of money each month to a company. Then, the company will help the person to pay for health care, like going to the hospital or getting medicine.
J
K
L
Legal Issues: These situations involve laws. A person might need help from a lawyer. In this study, legal issues were guardianship, wills and trusts
M
Mental health professionals: Trained people who help people with their mental health.
Medical Home: In a medical home, a team of medical providers manages your care. They listen to the patient to make sure they get the care they need. It is all about the patient.
Medical Providers: People or places that give medical care. This includes doctors, nurses or hospitals.
Mood Disorders:
N
O
Outcomes: Results.
P
Pap smear: A test where a swab is inserted into the vagina to check for abnormal cells.
Pediatric: Children under the age of 18.
Pediatricians: Doctors for children.
Policy: Rules people follow to know what to do. OR The ideas and beliefs used by a government or group when making decisions.
Post-secondary education: Opportunities to learn after high school. This can include trade programs, college, or any other learning opportunity.
Primary care: The medical office which is the main point of contact for a person’s medical care. It includes basic medical care like annual checkups and shots.
Preventative Healthcare: Healthcare that keeps you healthy, like regular check-ups and routine testing. Healthcare to prevent a condition from getting worse.
Privacy: There is a federal law that says a person decides who can look at and get a copy of your health information.
Q
R
Reactive Healthcare: Getting medical care after you are sick. Not getting healthcare, like a vaccine, to prevent an illness.
Rectal exam: Wearing gloves, doctor puts a finger into the patient’s rectum to feel some internal organs.
Resources- Adult: Information, services and supports just for adults.
S
Safer sex: Ways to prevent pregnancy and avoid sexually transmitted infections.
Screening: A test to find out if you have or are at risk for a health condition
Shared care: When a pediatric and an adult healthcare provider work together to care for a patient
Schizophrenia:
Seizures: A sudden electrical event in the brain
Self-care: Skills used to take care of yourself.
Sensory sensitivities: Being more aware of and sensitive to your environment. For example, more aware of and sensitive to smells, sounds, touch, brightness, quick moving.
Sexual Health and Wellbeing: the physical, emotional, and social aspects of expressing one’s sexuality.
Sexually transmitted infections (STI): Infections that you can get through sexual contact.
Shared Care: Medical care from a group of providers who work together to treat you
Social workers: A specialist who helps you meet your basic physical, mental and emotional health needs. Some do counseling. Some connect a person to services.
Special Educators: People who teach children with learning differences
Specialists: A healthcare provider who treats specific conditions, or works with a certain area of the body.
Supported decision making: Helping a person understand their choices and make their own decisions. Supported decision making is not like guardianship. With guardianship, the guardian makes decisions for the person.
Supporter or Support Person: Someone who may go with the person to appointments.
STI Testing: Medical tests to find out if you have a sexually transmitted infection.
T
Taking Blood Pressures: To measure how strong blood is moving from your heart through your your body
Telehealth or Telemedicine Visits: Meeting with your medical provider on a video call.
Transition Care Coordinator: The person who manages services for a patient moving into adult care.
Transition Services Program: Ways to help a child transition to adult services
Transportation: A way to get from one place to another.
U
V
Vocational programs: Support and training to help a person find and keep a job.
back to top
W
Waiting Room Environment: How a waiting room is set up to make a person feel welcome and comfortable.
X
Y
Important Topics for Healthcare Transition Research
During a first series of focus groups and during individual interviews we talked about 5 research articles and their models for healthcare transition.
Some of the guiding questions were:
- How do these models compare with your experience in Vermont?
- Which models or aspects of these models would be applicable to Vermont?
You told us about 8 important research topics for Vermont.
Select each topic for details and quotes from participants in our focus groups.
THEME 1: Training in autism is necessary for healthcare providers and staff, including mental health providers. Not enough time is spent on autism during medical school. Participants noted many topics to be included in training, such as:
- Support needs and the unique challenges of autism
- Conditions that co-occur with autism
- Gender-affirming care in the context of autism
- Early autism diagnosis
- Diagnosis in gender and age diverse populations
- Identification of autistic traits in those who choose not to disclose or do not know they might be Autistic
- Healthcare transition framework to support transition to adult care from pediatrics
One autistic youth described some of the training issues he has experienced:
“Because the people working for such a thing [healthcare] have not gone through the study of those on spectrum [or have] learn[ed] how to teach them [autistics] these skills in the right way to make sure their minds can keep up with the lesson that they’re trying to teach . . . forcing me to believe I need to be self-taught rather than taught by a professional.”
A parent shared their concerns on training needs:
“It’s the training too, for people that are providing the care. How do we get that to the folks so it becomes more automatic, not a freeze-in-place situation, and they don’t know what to do with your individual with these complex needs.”
A physician added their perspective on training:
“I know I don’t have too many patients who are like autistic, but I do have a few that I’ve met with and I mean, I have education from school, but I have no further training outside of just didactic work.”
THEME 2: Accessibility of care is important. This includes available trained providers, accommodations, and being able to find providers and resources.
Examples of accommodations noted include:
- Telehealth
- Visual supports
- Environmental changes to address sensory sensitivities
- Limiting waiting time
- Plain language
An autistic adult described important aspects of accessibility that were missing from her experience:
“I agree with […] having as much predictability is ideal and opportunity for easily accessible written communication with health care provider instead of having to jump through hoops to get answers, like my process of being diagnosed.”
Another autistic youth described her need for being heard. Lack of accessibility resulted in her avoiding going to her doctor:
“I feel like they don’t totally listen or like I feel like I’m not taken seriously when I talk about like concerns, so I really just try to go to the doctor as little as possible, because it can definitely be an issue. And then a lot of doctors sometimes like put things as oh, it’s because of a mental illness. It’s like, No, no, it’s not so. It definitely can be hard feeling like they’re not fully getting what I’m saying.”
A parent shared her experience with lack of sensory accessibility in healthcare:
“And once you move into adult care, especially if you’re raising a male, you really lose any sensitivity to the challenges that this individual is having moving through all of the sensory overload that they already have on top of the pain that they’re experiencing, and they present differently, because they get into that fight or flight mode, and it’s really hard to calm the panic down.”
THEME 3: Use an individualized, wrap-around approach with a transition framework that includes the autistic youth in making their transition plan.
This transition plan would include healthcare, mental health, education, employment, and community connection services/resources. Important parts of the transition plan include:
- Someone serving in a role of transition coordinator or supporter
- A warm hand-off to the new provider
- Help understanding how insurance and medical billing works
- Partnering with schools, designated agencies, and community organizations
One professional offered her view on the benefit of a transition manager:
“I think that there might be a role for something like a transition manager. But I’m not sure if situating it in just health care would be the best choice.”
A parent talked about her experience compared to transition support mentioned in the articles reviewed for the discussion:
“But, just there’s so much stuff, and I just, I don’t know anybody else’s experience, any of it. But I, there’s so much good stuff that could happen, and pre-planning, and I just haven’t seen any of it.”
THEME 4: All autistic youth and adults should have universal access to mental health support by autism-trained providers.
- Mental health care is also important for parents/caregivers.
- The parent-child relationship changes during the time of transition to adulthood requiring additional mental health support.
An autistic adult talked about the importance of specialized mental health supports:
“Access to different kinds of mental health services is sorely needed. Too often the only option on state insurance is CBT, which isn’t the most helpful for a lot of types neurodivergence. We need access to specialized care for the many conditions that are often comorbid with autism, like OCD.”
An autistic youth described their need for mental health support:
“I have had both negative and positive experiences [with mental health therapists]. And I do need a therapist to manage some of my issues, because I do not wish to trauma dump here, but I have been through some intense past experiences which I cannot process on my [own] or I prefer to process with someone else to talk to and filter through.”
A mother described difficulties in finding a mental health provider who was comfortable working with an autistic youth:
“But we had a whole string of counselors, social workers who really didn’t know how to interact with her or help her, and we tell me that they didn’t know anything about autism. Some providers didn’t want to see her when they heard that she had an autism diagnosis, and others just had no idea how to approach her.”
THEME 5: Preparing Autistics for adult healthcare should start as early as kindergarten. The autistic youth should be empowered in their autistic identity, disability rights, and making their own decisions.
- Autistics need to develop skills to take care of their healthcare needs.
- Education should include developing relationships, and understanding sexual health:
- Sexual health information should come from a source other than parents/caregivers.
- Social, mental, and physical health aspects of adult relationships should be addressed.
- Social safety and the prevention of relationship trauma are important topics to include.
One autistic youth described what he would like to see early on in health classes:
“So, sharing my opinion on how sex should be discussed. I am a sexually active trans gay man . . .I think that they should really talk about [it] in health class like how different relationships work safely with different contraception as well as just you know safety with actions and relationships… talking to other people and communicating openly about sexual, nonsexual [behavior]… I don’t think that being quiet about it, or hush, hush about it, or only talking about it with your parents and your very special teachers. I don’t think that’s smart or healthy.”
A professional explained how empowering autistic children to make decisions should start early:
“Transition starts at preschool. Transition starts with a paradigm of how do I empower my patient to learn about their brain, to learn about their access needs, to learn about self advocacy skills.”
A professional and disability advocate talked about the importance of knowing your identity to advocate for your rights for reasonable accommodations:
“We have that discussion about how we have to [help] our children to know who they are, because disability is part of our identity. Nobody can take that out from us, and the more we embrace it that we have it, the more we can move forward because it’s just one step to see. I have a disability. And that part of me, it’s just 1%. As I always say, the 99% has to be what developed by you yourself. […] we draw from having what we call reasonable accommodation because that is how the ADA [American with Disability Act] defines it. And then that makes you qualify to actually have all the services.”
THEME 6: Increase opportunities for both inclusive and autism-specific community engagement for Autistics.
- There is a need to increase understanding and visibility of autism across other identities: BIPOC (Black, Indigenous, and People of Color), disability, neurodiversity, and LGBTQ+ (Lesbian, Gay, Bisexual, Trans, Queer and more) communities.
An autistic youth shared their desire for connection and a way to engage around shared interests while accommodating different needs:
“… just have like a way to get people together and socializing with people similar to them in a way that’s like really accommodating towards other people’s needs because everybody’s needs aren’t the same . . .because I know I’ve struggled personally with finding and making friends, especially because I’m online school and Vermont is just not a place with a bunch of different things like that.”
An autistic adult described opportunities for creating inclusive communities:
“I think we really need to tap into groups like Outright and the local Pride organizations. They have special groups for transgender people. They have special groups for gay men. They have special groups for other subculture parts of the LGBTQ community. And I think that it will be a really positive thing if these organizations actually catered also to the autistic community as a part of the subculture, because we’re six times more likely to be a part of that community than the neurotypical population.”
A mother described an additional benefit of promoting inclusive communities:
“The other thing is, our kids help educate their community if they’re included.”
THEME 7: Developing a trusting relationship with providers is essential. It takes time. Autistics want to feel like their provider cares about and understands them.
- Beginning the transfer of care early or to a family practitioner would help develop a relationship by the time youth become adults.
- Options to build relationships could include telehealth, home visits, open houses, or co-visits with their pediatrician.
One autistic respondent described his approach to building a relationship with his healthcare provider:
“One idea I have right now is to start off by having a long distance conversation with the doctor until you feel more comfortable around them. . . . I would prefer to be seen from a long distance video chat. And then, and once you’ve gotten to know that person a little, well get to know them in person: before reaching out to your more medical and mental needs like basically take it like one saying, I have, take it like I haven’t used this one in a really long time. But I some on rare occasions I use, like to say, take it as slow as a sloth.”
An autistic mental health professional shared about lack of trust and the need to feel safe:
“I know that there is a requirement in order to have your first visit for you to transfer your records to a new provider so they have every bit of information they can possibly see about you before they meet you. And that’s a role for so many practices right now. We need to be able to know if it’s a good fit or if it’s going to be a safe space. And we have a lot of private information about ourselves. Doctors, they don’t get to have that because they want to.”
THEME 8: The healthcare and support services structure does not support providers and patients in meeting their healthcare and mental health needs.
- Lack of a support service structure affects healthcare transition needs.
- Complex insurance issues and payment structure are barriers to access care and to collaboration for healthcare transition.
- Care coordination has been identified as an important priority for funding.
A parent of an autistic adult, and a community-based professional, described the barriers to healthcare:
“I was thinking about how most providers don’t understand the way we bill for health care in the United States. But when you make your appointment it’s like you get this approximately 10 to 15 min window . . . You know, as someone who is neurotypical that’s not enough time for me to give like the context and the detail to my physician about what I’m experiencing, what are potential solutions and having a dialogue with my physician. And so, if I imagine, my son, as an adult going into those conversations and knowing that he’s very detailed-oriented, and he wants to give it a whole context. I think one of the key things to think about is [the] idea of the longer appointment times and making sure physicians are positioned in the healthcare billing system for that, because it is meeting the patient’s needs by giving them an extended window of time.”
An autistic adult described the need for insurance to cover mental health:
“… I mean health insurance is a whole other beast. But I think, making sure that it’s clear that, especially for autistic people, mental health is as essential, mental health care is as essential as like physical care, but that shouldn’t be like some extra cherry on top that you get. If your insurance happens to pay for it, or what like that, that needs to be included in the whole package.”
One interesting finding was that the important research topics were similar across the focus group discussions and the interviews. They were also similar between autistic and non-autistic participants.
For information on how we came to these results visit the method page on this website.
Measuring Important Research Outcomes
During a second series of focus groups we talked about important research outcomes.
We reviewed the outcomes measured in the 5 research articles discussed in the first focus group as examples to guide our discussion.
Some of the guiding questions were:
- How would we know the transition supports are working?
- How would it make a difference in your experience?
All the research outcomes below were clearly important to the project participants and survey respondents.
- 6 research outcomes were rated as higher priority.
- 10 research outcomes were rated as medium priority.
- There was no clear data to identify lower priority outcomes.
We would know that healthcare transition research has an impact when…
Autistic youth and adults would experience:
Better quality of life
- Connections with people that matter to the autistic person
- Involvement in areas of life that matter to the autistic person
- Continuity of daytime activities after High School (education, employment, recreation, etc.)
- Improved relationship with parents/caregivers and family
- Social networks and supports outside of providers exist if desired
- Comfort to express themselves romantically/sexually in relationships
Better mental and physical health
- Less physical and mental health emergencies
- Less trauma, depression, suicidality, addiction
- Increased lifespan
- Less secondary complications from lack of care
- Less unplanned pregnancy, sexually transmitted diseases
- Well managed medical conditions
- Increased feeling of self-worth
- More self-regulation experienced
More physical and mental healthcare needs are met
- Autistics have an autism-informed provider and specialists
- Preventative care is received (immunization, cancer screens, teeth cleaning, eye exam, etc.)
- Visit goals are met
- Continuity of care and treatment occurs before, during and after transition
- Autistic youth and their parents/caregivers have energy left for other areas of life
- Referrals are made for unresolved health concerns
- Less time needed for diagnosis, treatment, improvement of symptoms
More independence with healthcare
- Healthcare accommodations and supporters are available as needed
- Parents/caregivers can step back as the primary healthcare resource
- Autistics advocate and trust their intuition about their health needs
- Autistics understand the information shared about their healthcare needs
- Autistics develop better healthcare skills to meet their needs (taking meds, making appointments, etc.)
Improved relationship with provider
- Feeling heard, valued, empowered
- Having a good match with providers
- Attending scheduled visits
- Building partnerships with providers
- Feeling less of being a burden to others when getting needs met
- Sharing health concerns more candidly
More comfortable with healthcare visits and procedures
- Less stress and anxiety with healthcare visits and procedures
- More accessibility needs are met
- Less medical or physical restraint when getting healthcare
More providers would show:
Increased COMPETENCY in working with autistic people
- Better understanding of the features of autism in real life
- Improved anticipation of the healthcare needs of autistic patients
- More positive attitudes towards autistic patients and their caregivers
- Less biases towards autistic patients and their caregivers
- More autistic staff and providers working in health practices
- Increased number of autistic patients
- More referral from autistics and their caregivers
Increased BELIEF in their ABILITY to work with autistic people
Including perception of:
- Adequate training
- Adequate time and practice resources
- Quality of relationship with autistic patients
- Knowledge of where to refer autistic patients for appropriate care and services
The use of a menu of autism-informed accessibility options
Including:
- Pre-planning of visits
- Communication, environmental and sensory accommodations
- Offered to all patients, without the need to request them
- Home visits, telehealth, open-house
- Accessible information on autistic health
- Accessible information on health conditions and treatments
Active work to improve autistic people’s healthcare experience
- Positive relationship quality between provider and Autistics and their caregivers
- Responsive to feedback
The healthcare system would have:
More autism-trained providers available to take patients
Including more autism-informed providers who:
- Take Medicaid
- Work in a certified Medical Home (offering care coordination)
- Can see people the same day
- Will diagnose autism across the lifespan, cultures and gender identities
- Provide gender affirming care that is autism-informed
- Have interactions with autistic people in the community
- Are Autistic themselves
More autistic youth and adults with insurance coverage that meets their physical and mental health needs.
Increased access to autism-informed transition PLANNING
- More autistic youth have a comprehensive transition plan developed with their input
- The plan achieves the autistic person’s goals
- More transition plans demonstrate team collaboration across areas of function(education, employment, healthcare, independent living, community, etc.)
- More Individualized Education Plans (IEPs) and 504 plans have healthcare transition goals
Increased access to autism-informed transition SUPPORTS
- More autism-trained providers offer transition care and use a transition framework
- More providers assess transition readiness and successful completion of transition
- More school nurses support healthcare transition needs
- More autistic youth have access to an autism-informed support person for the transition process (e.g., care coordinator/ transition manager/patient navigator)
More specialized clinics in autism/neurodiversity or in “complex care” for adults with autism
More autistic-informed training options for Vermont providers
Including:
- More hours of autistic-informed training for students in medical, mental, allied health and education programs
- More autistic students in medical, mental health, allied health and education programs.
Opportunities and Allies
The Autism Collaborative has been fortunate to connect with key stakeholders in our efforts to understand their perspectives on research needed to address healthcare transition in Vermont. Autistic and non-autistic leaders, researchers, clinicians, caregivers and youth have identified a number of opportunities and allies for taking the next steps to improve healthcare transition for autistic youth and young adults.
- Vermont Child Health Improvement Program (VCHIP) works with clinics offering transition supports and transition tools.
- Emergency Room model to plan visits ahead of time with local physician champion.
- Pediatric “Comfort Zone” as model for specialized clinic for adults with autism or developmental disabilities.
- Directory of autism-trained providers.
- Education on transition and neurodiversity through community partners (Green Mountain Self-Advocates, Vermont Family Network, Vermont Center for Independent Living, All Brains Belong VT).
- Healthcare Navigator role similar to what is done for some Cancer Centers.
- Coordination between existing transition plans and transition managers (designated agencies, school plans, HireAbility, and healthcare providers).
- Practices already providing care coordination and training to providers (Qualified Health Centers, Appletree Bay Primary Care, All Brains Belong VT).
- “Hub and Spoke” model from the Vermont opioid project as an example to disseminate autism-informed care across Vermont.
- Got Transition resources for value-based payment for transition supports.
- Got Transition resources for increasing primary care access for adults with complex care needs.
- Network of community resources in Vermont who already work with youth (Outright Vermont, Umbrella, Youth Bureau, etc.).
- Vermont Child Health Improvement Program (VCHIP) is spearheading several healthcare transition projects. They are implementing the Got Transition recommendations. They have established transition collaboration projects with 7 clinics including pediatrics, family practice and internal medicine providers.
Tools developed:
o Materials to support patients and families.
o Chatbot to guide youth through the transition journey.
o Transition assessment added to the electronic health records.
o A “complex care” information section in the electronic record.
The lessons learned, tools and strategies put in place in their projects may have relevant applications for transition planning for autistic youth.
- The Emergency Department (ED) at the University of Vermont Medical Center (UVMMC) has a physician champion for improving the care of individuals with disabilities in that setting.
- Preparing for ED visits when needed for autistic patients, their families and providers should be part of the transition planning process.
- A model and planning tools exist for preparing families, autistic patients or patients with cognitive or communication differences and providers for ED visits to improve the experience of the autistic patient.
- A model of care using designated scheduling for children with complex care needs and the establishment of a pediatric ‘Comfort Zone’ for medical procedures have been used at UVMMC.
- For many pediatric patients there is a need for coordination of dental work, blood work and vaccines that are done under sedation but there are limits to how often and when this should be done.
- The Comfort Zone helps reduce the level of sedation required for medical procedures but there is currently no equivalent for adults with IDD/complex needs.
- A physician champion for individuals with IDD has submitted a proposal to fund the equivalent of a ‘Comfort Zone’ for adults with IDD including those with autism.
- Creating a directory of autism-informed providers and their different specialties would make it easier to make referrals, and for autistic individuals and caregivers to find a good match for the care needed.
- The Vermont Family Network (VFN) can be leveraged to provide information and education to parents. They have been a consistent partner in our PCORI projects and with VCHIP. The Vermont Center for Independent Living (VCIL), Green Mountain Self-Advocates (GMSA) and All Brains Belong VT are other excellent resources for educating autistic youth and their caregivers on disability and neurodiversity identity and on their protected rights.
- There is a model for patient navigators that has been established in the Cancer Center at Central Vermont Medical Center. This model is promising for transitioning from pediatric to adult care for autistic patients and could be funded by insurance if the provider was a licensed social worker.
- The role of current transition and care coordinators and transition plans that occur through schools, HireAbility, the designated developmental agencies and community health centers could be leveraged to facilitate healthcare transition. This would require greater collaboration and coordination among these agencies. Adding healthcare transition to those plans and making it easier to share information while respecting the different rules is needed.
- Apple Tree Bay is a UVM nurse practitioner faculty practice providing healthcare to patients 12 years and older through a certified medical home model. They provide a holistic, integrative health approach with care coordination, functional medicine, motivational interviewing, acupuncture, and massage among many services. They would be an ideal partner to initiate education for their practitioners and the students who participate as learners in the practice about autism specific accommodations and transition support.
- Currently, there is a hub and spoke model for opioid treatment in Vermont that has been very successful in meeting patients’ and providers’ needs in rural communities. Lessons learned from the model and the experience with implementation could help with future efforts to develop and disseminate autism specialized care across the state of Vermont.
- Vermont has many Federally Qualified Health Centers where providers work together and use the “medical home model” of care. The federal certification requires that these practices provide care coordination. It also requires training for providers. The Bi-State Primary Care Association provides technical assistance to these practices. Collaborating with this organization and with champions in this network would provide opportunities to disseminate training on autism friendly practices and implement transition supports.
- Got Transition has excellent guidelines for implementing a value-based payment initiative for transitioning from pediatric to adult primary care that can be a roadmap for Vermont’s efforts to develop a robust healthcare transition plan for autistic youth and adults.
- Got Transition also has a resource on ways to strengthen the adult healthcare workforce to support adults with complex care needs: Three models of complex care for adults are mentioned which have relevance and could be implemented in Vermont:
1) Enhanced primary care where current primary care practices increase their provision of interdisciplinary primary care, case management and disease self-management;
2) Transitional care focusing us on episodic care during transitions between the hospital and rehabilitation or home care; and,
3) Integrated care where there are cross disciplinary providers integrating their services for social, behavioral, medical, and overall health care.
- Finally, Vermont is rich in community resources such as the Youth Service Bureaus/Boys and Girls clubs, Outright Vermont, Pride, Umbrella (a violence and abuse prevention group), advocacy groups, recreational communities, etc. who do wonderful work with youth. They could be leveraged so they are part of a larger network or system of transition support that autistic youth and adults could access.
Who joined the discussions?
Stakeholders
A total of 56 stakeholders joined this project:
-
- 39 stakeholders attended the focus group discussions.
- 17 professionals were interviewed separately.
The stakeholders included 20 autistic participants:
-
- 9 autistic participants were youth aged 16 to 25 years.
- 11 autistic participants were adults aged 26 and older:
- 2 autistic participants were professionals;
- 1 was an autistic parent/caregiver, and
- 2 were both autistic parents/caregivers and professionals.
There were 26 non-autistic participants:
-
- 19 were part of the focus groups
- 17 were interviewed.
Focus group participants
Figure 1. Identities of focus group participants

Figure 2. Ages of autistic participants
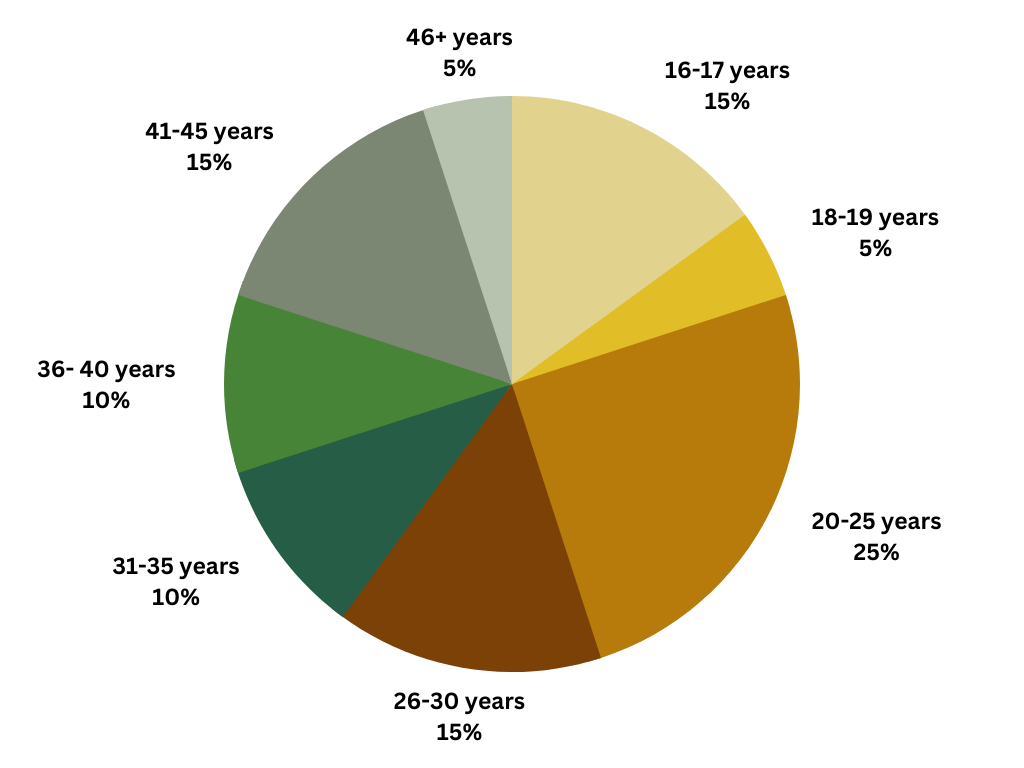
Figure 3. Autistic Identities by Age Group
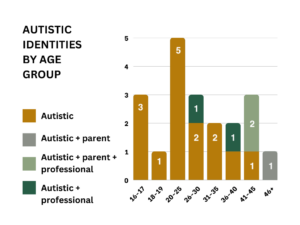
Table 1
| Professions | Number | Works with children | Works with adults | Works with both |
|---|---|---|---|---|
| Mental health | 4 | 1 | 1 | 2 |
| Psychiatrist | 1 | 1 | ||
| Nurse practitioner | 1 | 1 | ||
| Family physician | 1 | 1 | ||
| Special education | 2 | 2 | ||
| Health care facilitator | 1 | 1 | ||
| Home health | 1 | 1 |
Interview participants
The 17 non-autistic professionals interviewed included:
- Physicians representing:
- Pediatrics
- Family practice
- Internal medicine
- Emergency department
- Anesthesiology
- Pulmonology
- Gender affirming care
- Professionals from the Vermont Child Health Improvement Program (VCHIP).
- Patient-centered care support service specialists.
- Healthcare navigator.
- Representative from a designated developmental agency
- HireAbility transition specialist.
- Vermont Center for Independent Living (VCIL) representative.
This project was fully funded through a Patient-Centered Outcomes Research Institute (PCORI) Eugene Washington PCORI Engagement Award EASCS-24099
- Covert, S. (2016). The Inclusive Healthcare Partnership Project -Removing the Barriers: Improving Health Care for Adults Vermonters with Developmental and Intellectual Disability.
- Kuhlthau, K.A., Delahaye, J., Erickson-Warfield, M., Shui, A., Crossman, M., & van der Weerd, E. (2016). Health care transition services for youth with autism spectrum disorders: Perspectives of caregivers. Pediatrics, 137(S2), e20152851N.
- Rast, J.E., Shattuck, P.T., Roux, A.M., Anderson, K.A., & Kuo, A. (2018). The medical home and health care transition for youth with autism. Pediatrics, 141(4), 5328-5334.
- Nathenson, R.A., & Zablotsky, B. (2018). The transition to the adult health care system among youths with autism spectrum disorder. Psychiatric Services, 68(7), 735-738.
- Stringer, E.T., Ortiz Aragon, A. (2021) Action Research 5th Edition. Sage Publications. Thousand Oaks, California.
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77-101.
- Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11(4), 589-597.
- Braun, V. & Clarke, V. (2021). Thematic analysis: A practical guide. Sage.